| 
 |
|
There are a number of endocrine conditions that may emerge during pregnancy. Diabetes and thyroid disorders are the most commonly encountered problems. Fortunately, with careful management, potential risks associated with these conditions are largely avoidable.
Gestational diabetes
Gestational diabetes mellitus (or GDM) is a form of diabetes that comes on in pregnancy. It is usually detected on routine glucose tolerance test (GTT) at the end of the second trimester (high risk women should have a test earlier on). The GTT involves having a sugary drink (75gram of glucose), then having a blood test at the start and after 1 and 2 hours have elapsed.
Gestational diabetes is becoming more common in Australia and now affects around 1 in 10 pregnancies. It is becoming more common partly due to the older age that women are having babies and also due to the trend towards people being more overweight (60% of Australian adults are now classified as overweight or obese).
Gestational diabetes carries a number of potential risks for mother and baby. Babies to diabetic mothers are more likely to be large and in particular have large heads (called macrosomia) which can make vaginal delivery more difficult. There is increased risk of premature delivery, miscarriage and the need for caesarean section. The baby may develop low blood sugar level after delivery and therefore should be monitored closely after the delivery. Fortunately, if the diabetes is well controlled many of these potential risks can be avoided.
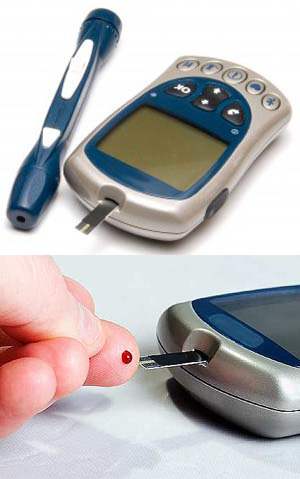
Management of diabetes involves following a healthy diet, aimed at providing small amounts of carbohydrate consistently (ideally low glycaemic index) and avoiding excessive weight gain. To assess the success of diet fingerprick blood glucose levels need to be monitored, up to four times each day. If blood sugars are high despite adherence to the diet then medication in the form of tablets or injected insulin may be required.
Gestational diabetes almost always resolves after delivery, however it is an important indicator of elevated future risk for type 2 diabetes and hence great care should be taken to adopt a healthy lifestyle aimed at maintaining a healthy weight.
Thyroid disorders in pregnancy:
Thyroid problems in pregnancy are very common, but fortunately usually easy to manage.
Iodine
Adequate iodine intake in pregnancy is important for baby's development, especially in the first trimester. Pregnant women are recommended to include 250mcg of iodine in their daily intake - most will require a supplement to achieve this.
Hypothyroidism
Hypothyroidism is common, affecting around 1 in 20 pregnancies. The symptoms of hypothyroidism (fatigue, constipation, feeling cold) are common in normal pregnancies and therefore difficult to recognise. Many women with hypothyroidism don't have any symptoms and so it may be incidentally picked up on a routine blood test.
Untreated hypothyrodisim carries potential risks of reduced fertilty (difficulty getting pregnant), miscarriage and impaired intellectual development in the baby. Thyroid hormone can be given safely during pregnancy and the dose adjusted based on regular blood tests.
Hashimoto's disease
Hashimoto's is the most common cause of hypothyroidism is Australia. It is one of the auro-immune forms of thyroid disease where the immune system produces anti-bodies that attack the thyroid gland and may interfere with its normal function. These antibodies are readily detected on simple blood test. Around 1 in 10 women have thyroid antibodies detected. If antibodies are detected, there is some evidence that a small dose of thyroid hormone replacement may reduce the risk of miscarriage, even when thyroid function is normal. If blood test reveal an underactive thyroid, then hormone replacement should be commenced immediately and will often need to be continued lifelong.
Hyperthroidism (thyrotoxicosis)
Hyperthyroidism is relatively uncommon in pregnancy. Grave's is the most common cause of hyperthyroidism in pregnancy and can usually be controlled with just small doses of anti-thyroid medications. Some women with mild Grave's disease won't require any medication at all and can simply be monitored with regular blood test.
Women with hyperemesis gravidarum (extreme vomiting of pregnancy) may also develop abnormal thyroid function tests suggestive of thyrotoxicosis, but this usually doesn't require anti-thyroid medication.
 |